What can be done for the condition?
The treatment of OA of the ankle can be divided into the nonsurgical means to control the symptoms and the surgical procedures that are available to treat the condition. Surgery is usually not considered until it has become impossible to control the symptoms without it.
Non-surgical Rehabilitation
Rehabilitation services, such as those offered at Momentum Spine & Sport Physiotherapy, play a critical role in the treatment plan for ankle joint arthritis. Treatment usually begins when the ankle first becomes painful. The pain may only occur at first with heavy use and may simply require the use of mild anti-inflammatory medications such as aspirin or ibuprofen. Reducing the activity or changing from occupations that require long periods of standing and walking may be necessary to help control the symptoms.
The main goal of your physiotherapy program is to help you learn how to control symptoms and maximize the health of your ankle. Our therapist will instruct you on techniques you can use to calm your pain and symptoms. We may advise may use rest, heat, or topical rubs. Our physiotherapist will work with you to improve flexibility, balance, and strength. Our physiotherapist in Edmonton and St Albertwill also provide training to help you walk smoothly and without a limp, which may require that you use a walking aid such as a walker, crutches, or cane.
Braces that reduce the motion in the ankle can also be beneficial in reducing pain. Special braces that transfer some of the body weight to the knee can help protect the ankle. These braces are called patellar tendon bearing braces. They are quite large and bulky and may not be well tolerated by some patients.
We may recommend modifying your shoe with a rocker sole may give some relief of symptoms. The rocker sole replaces your normal sole with a rounded one, allowing your foot to roll as you move through a step. This can help take stress off the ankle as you walk.
If you don't need surgery, we may recommend that range-of-motion exercises for the ankle be started as pain eases, followed by a program of strengthening. Our program then advances to include strength and balance exercises. Your physiotherapist will give you tips on keeping your symptoms controlled. Although recovery time varies among patients, as a guideline, you may progress to a home program within four to six weeks.
In cases of advanced OA where surgery is called for, patients may also see our physiotherapists before surgery to discuss exercises that will be used just after surgery and to begin practicing using crutches or a walker.
Post-surgical Rehabilitation
Your ankle will be bandaged with a well-padded dressing and a splint for support after surgery. Most patients are instructed not to place weight on their foot for a period of time after surgery. After arthroscopy, this period typically lasts about one week. Although recovery time is not the same for everybody, after ankle joint replacement, most patients are usually advised to avoid placing weight on their foot for up to 12 weeks.
Physiotherapy sessions, such as those provided by Momentum Spine & Sport Physiotherapy, may be needed after surgery for up to two months. When you visit Momentum Spine & Sport Physiotherapy, your first few treatments will be used to help control the pain and swelling after surgery. Treatments provided by our therapist may include electrical stimulation, ice, and soft tissue massage. We may also use hands-on joint movements and stretching to improve your range of motion and flexibility.
Our physiotherapists sometimes treat patients in a pool. Exercising in a swimming pool puts less stress on the ankle joint, and the buoyancy lets you move and exercise easier. Once you've gotten your pool exercises down and the other parts of your Momentum Spine & Sport Physiotherapy rehab program advance, you may be instructed in an independent program.
Our physiotherapist will also work with you to safely increase the amount of weight you are able to place on your foot. Our goal will be to help you walk comfortably and with a smooth walking pattern. Some of the exercises you'll do are to help strengthen and stabilize the muscles around the ankle joint. Your physiotherapist will provide tips on ways to do your activities while avoiding extra strain on the ankle joint.
Momentum Spine & Sport Physiotherapy provides physiotherapy services in Edmonton and St Albert.

 Injury to a joint, such as a bad sprain or fracture, can cause
Injury to a joint, such as a bad sprain or fracture, can cause 
 An
An  The
The 
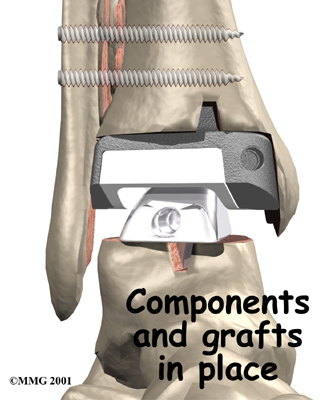 Because no one wants to lose the ability to move the ankle, much research has been done trying to perfect an
Because no one wants to lose the ability to move the ankle, much research has been done trying to perfect an 