After hip arthroscopy rehabilitation at Momentum Spine & Sport Physiotherapy should begin as soon as possible. There are a few cases where your surgeon may delay a start in your therapy because they want the tissues to heal with rest before any further stress is placed on the hip. Often therapy begins before you are even allowed to fully weight bear. In other cases, rehabilitation will not be recommended until full or nearly full weight bearing begins. Each surgeon will set his or her own specific restrictions based on what was done during the surgical procedure, their personal experience, and whether your tissues are healing as expected. Generally speaking, the more complex the surgery the more involved and prolonged your rehabilitation program will be.
If you are still using crutches by the time we first see you at Momentum Spine & Sport Physiotherapy, your physiotherapist will ensure you are using the crutches safely, properly, and confidently and that you are abiding by your weight bearing restrictions. We will also ensure that you can safely use your crutches on stairs. If you are no longer using crutches, or once you no longer need them, your physiotherapist will focus on normal gait re-education so you are putting only the necessary forces through the surgical side with each step, and are not compensating in any way. As mentioned above, until you are able to walk without a significant limp, we recommend that you continue to use your crutches, or at least one crutch or a cane/walking stick. Improper gait can lead to a host of other pains in the knee, hip and back so it is prudent to use a walking aid until near normal walking can be achieved. Your Momentum Spine & Sport Physiotherapy physiotherapist will advise you regarding the appropriate time for you to be walking without any walking aid at all.
During your first few appointments at Momentum Spine & Sport Physiotherapy your physiotherapist will focus on relieving the pain and inflammation from the surgical procedure itself. We may use modalities such as ice, heat, ultrasound, or electrical current to assist with decreasing any pain or swelling you have around the surgical site or anywhere down the extremity. In addition, your physiotherapist may massage your leg and ankle to improve circulation and help decrease your pain.
The next part of our treatment will focus on regaining the range of motion in your hip. Your physiotherapist at Momentum Spine & Sport Physiotherapy will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of a home exercise program. Range of motion in the hip generally comes back very quickly after an arthroscopic surgery, but it still depends on what your surgeon has done inside your joint. Most often patients find their range of motion improves slightly from prior to surgery because their surgeon has cleaned up the joint. You may experience a small amount of discomfort at the end ranges of motion initially, but it is still important to perform the range of motion exercises that your therapist prescribes because moving the joint also helps to move the swelling, get fresh blood to the healing area, and provide nutrition to the surface of the joint. Only mild discomfort, however, is permissible. Any sharp or moderate discomfort should be heeded. An exercise bike at this stage is very useful to assist in gaining back the hip flexion and extension range of motion. Even if you are unable to fully rotate the pedals of the bike it is still encouraged as performing the back and forth motion forces fluid through the joint and greatly assists the healing process.
If necessary your physiotherapist will mobilize your hip joint. This hands-on technique encourages the hip to move gradually into its normal range of motion. Mobilization of the hip may be combined with assisted stretching of any tight muscles around the surgical site.
At Momentum Spine & Sport Physiotherapy we also highly recommend maintaining the rest of your body’s fitness with regular exercise while your hip is healing. This can begin very early post-surgically. You can use an upper body bike if you are non-weight bearing or may even be allowed to do non-weight bearing exercises in a pool. A stationary bike is often the best cardiovascular activity once weight bearing begins and your range of motion allows it. Weights for the upper extremities and other leg are also strongly encouraged. Your physiotherapist at Momentum Spine & Sport Physiotherapy can provide a program for you to maintain your general fitness while you recover from your surgery.
As soon as possible your physiotherapist will prescribe strengthening exercises. These exercises will focus on the muscles of your hip and thigh but will also include some exercises for your back as it plays a large supporting role for your hips. Exercises that involve the entire lower limb, such as squats, will also be given. It is important for you to perform weight bearing exercises as soon as you are able to in order to build up the muscles in a functional position, such as standing. Exercises that work the muscles while in standing most effectively assist with daily activities such as walking and stair climbing. Other exercises in sitting or lying, however, may also be prescribed. Exercises in these positions can be excellent in allowing you to target specific muscles around the hip, such as the gluteals, without causing you any discomfort from too much body weight being on the hip. Your therapist may use an electrical muscle stimulator to assist your muscles in contracting as you do your exercises; this will help you to more rapidly gain your strength back. Exercises may also include the use of Theraband or weights to provide some added resistance for your hip and lower extremity. If you have access to a pool, your therapist may suggest you go to the pool to do your exercises. The buoyancy of the water along with the warmth of the water can assist greatly in providing comfort to the hip joint and often allows your exercises to be done more easily with less discomfort.
As a result of any injury, the receptors in your joints and ligaments that assist with balance and proprioception (the ability to know where your body is without looking at it) decline in function. A period of immobility and reduced weight bearing will add to this decline. If your balance and proprioception has declined, your joints and your limb as a whole will not be as efficient in their functioning and the decline may also contribute to further injury in the future. As a final component of our treatment your physiotherapist at Momentum Spine & Sport Physiotherapy will prescribe exercises for you to regain this balance and proprioception. These exercises might include activities such as standing on one foot or balancing on an unstable surface such as a wobbly board or a soft plastic disc. Advanced exercises will include agility type exercises such as light hopping or moving side to side.
As your range of motion, strength, and proprioception improve, your therapist will advance your exercises to ensure your rehabilitation is progressing as quickly as your body allows. As soon as it is safe to do so, your physiotherapist will add more aggressive exercises such as jumping, hopping, and running, or exercises that mimic the sports or recreational activities that you enjoy participating in. During all of your exercises you therapist will pay particular attention to your technique to ensure that you are not using any compensatory patterns or are developing bad habits in regards to how you use your hip and lower extremity.
Enduring pain in your hip for years, months, or even just weeks generally causes you to use your hip and lower extremity in a pattern that avoids or limits your pain, but that is not efficient for a normal hip. If you do not pay close attention to how you use your joint and limb post-surgically these patterns often continue to occur once the source of your pain has been eliminated by the arthroscopic surgery. Your physiotherapist at Momentum Spine & Sport Physiotherapy will be crucial to providing you with feedback regarding correcting these patterns and developing new, efficient patterns during your daily activities.
Today, the arthroscope is used to perform quite complicated major reconstructive surgery using very small incisions. Remember, however, that just because you have small incisions on the outside, there may be a great deal of healing tissue on the inside of the hip joint. If you have had major reconstructive surgery, you should expect full recovery to take several months.
Generally the rehabilitation after arthroscopic hip surgery responds very well to the physiotherapy we provide at Momentum Spine & Sport Physiotherapy. If for some reason, however, your pain continues longer than it should or therapy is not progressing as your physiotherapist would expect, we will ask you to follow-up with your surgeon to confirm that the hip is tolerating the rehabilitation well and ensure that there are no complications that may be impeding your recovery.
Momentum Spine & Sport Physiotherapy provides services for physiotherapy in Edmonton and St Albert.
Portions of this document copyright MMG, LLC.
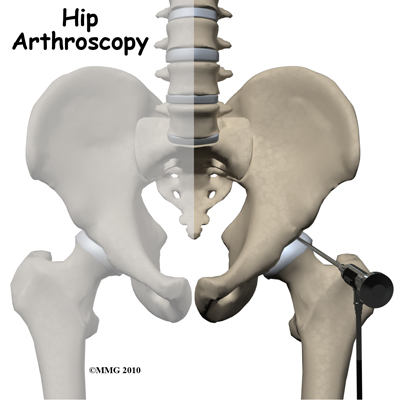
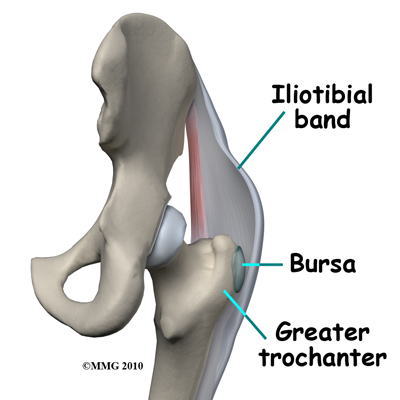
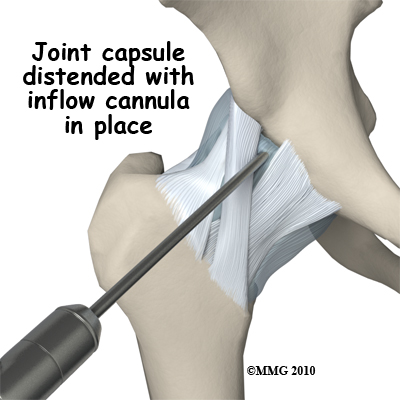
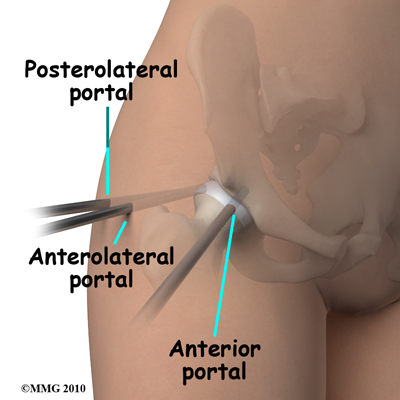
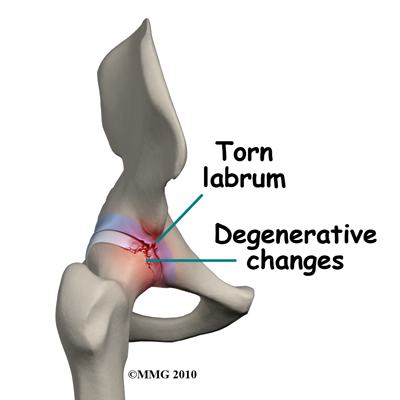 When hip arthroscopy first became available it was used primarily to look inside the hip joint and make a diagnosis. Today, hip arthroscopy is used in performing a wide range of different types of surgical procedures on the hip joint including confirming a diagnosis, removing loose bodies, removing or repairing a torn labrum, debriding excess inflamed bursa tissue, repairing a tear in the gluteus medius tendon and fixing fractures of the joint surface.
When hip arthroscopy first became available it was used primarily to look inside the hip joint and make a diagnosis. Today, hip arthroscopy is used in performing a wide range of different types of surgical procedures on the hip joint including confirming a diagnosis, removing loose bodies, removing or repairing a torn labrum, debriding excess inflamed bursa tissue, repairing a tear in the gluteus medius tendon and fixing fractures of the joint surface.
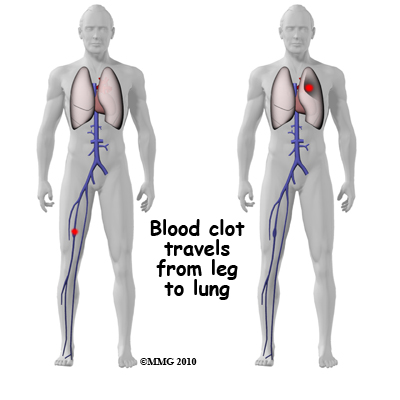 Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when blood clots form in the large veins of the leg. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lungs, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective way is to get you moving as soon as possible after surgery. Moving means getting you up out of bed to sit in a chair and to walk as soon as you are able, but it also includes having you perform ankle circles and ankle pumping exercises while lying down or sitting, which also helps to keep the fluid moving in your legs. Two other commonly used preventative measures include pressure stockings, as described above, and medications that thin the blood and prevent blood clots from forming.
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when blood clots form in the large veins of the leg. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lungs, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective way is to get you moving as soon as possible after surgery. Moving means getting you up out of bed to sit in a chair and to walk as soon as you are able, but it also includes having you perform ankle circles and ankle pumping exercises while lying down or sitting, which also helps to keep the fluid moving in your legs. Two other commonly used preventative measures include pressure stockings, as described above, and medications that thin the blood and prevent blood clots from forming. 