Physiotherapy in Edmonton and St Albert for Mid Back
Welcome to Momentum Spine & Sport Physiotherapy's patient resource about Thoracic Disc Herniation.
A rise in the use of magnetic resonance imaging (MRI) has led to the discovery that many people, perhaps as many as 15 percent of Americans, have a thoracic disc herniation. Seeing a herniated thoracic disc on MRI is often incidental, meaning it shows up when the person has MRI testing for another problem.
Few people with a thoracic disc herniation feel any symptoms or have any problems as a result of this condition. In rare cases when symptoms do arise, the main concern is whether the herniated disc is affecting the spinal cord.
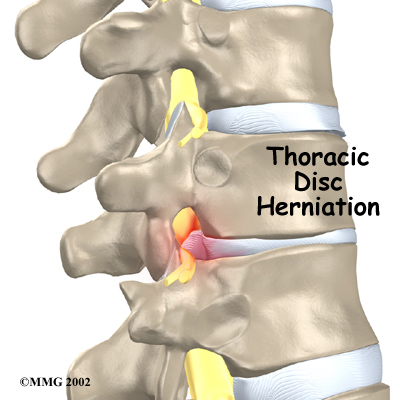
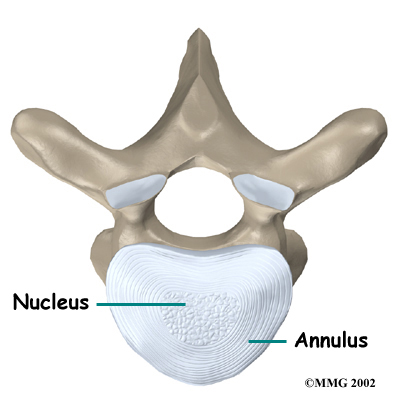
Although people often refer to a thoracic disc herniation as a slipped disc, the disc doesn't actually slip out of place. Rather, the term herniation means that the material in the center of the disc has squeezed out of the normal space. In the thoracic spine, this condition mostly affects people between 40 and 60 years old.
This guide will help you understand:
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Back Pain|limit:15|heading:Hear from some of our patients who we treated for *Back Pain*#
 The
The 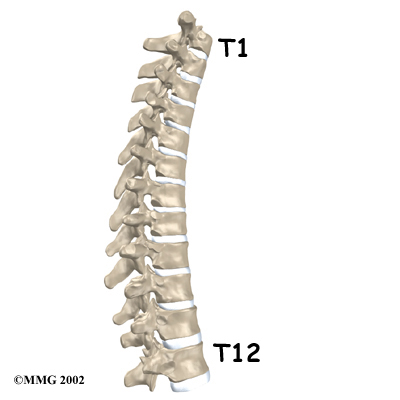
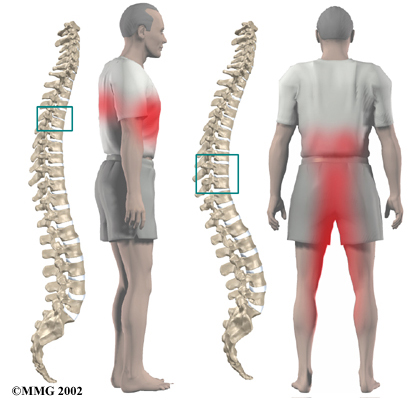
 The upper half of the thoracic spine is much less mobile than the lower section, making disc herniations in the upper thoracic spine rare. About 75 percent of thoracic disc herniations occur from T8 to T12, with the majority affecting T11 and T12.
The upper half of the thoracic spine is much less mobile than the lower section, making disc herniations in the upper thoracic spine rare. About 75 percent of thoracic disc herniations occur from T8 to T12, with the majority affecting T11 and T12.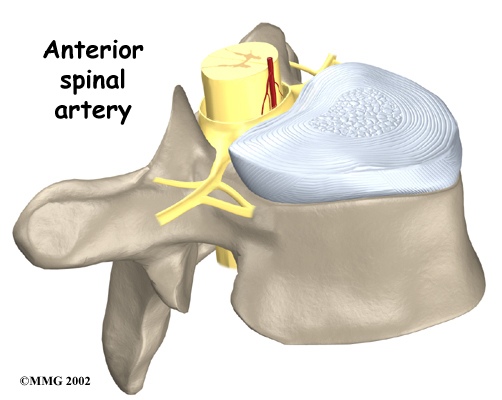
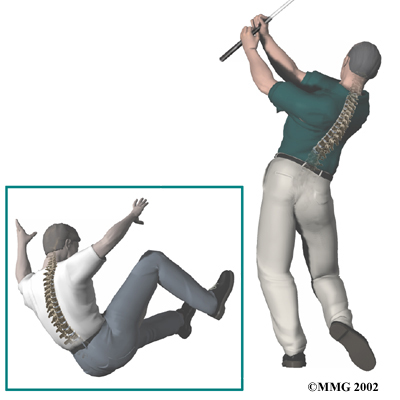 Less commonly, a thoracic disc may herniate suddenly (an acute injury). A thoracic disc may herniate during a car accident or a fall. A thoracic disc may also herniate as a result of a sudden and forceful
Less commonly, a thoracic disc may herniate suddenly (an acute injury). A thoracic disc may herniate during a car accident or a fall. A thoracic disc may also herniate as a result of a sudden and forceful