What treatment options are available?
Whenever possible, doctors treat biceps tendonitis without surgery. Anti-inflammatory medicine may be prescribed to ease the pain and to help patients return to normal activity. These medications include common over-the-counter drugs such as ibuprofen.
A crucial part of non-conservative treatment for biceps tendonitis is physiotherapy treatment.
Physiotherapy at Momentum Spine & Sport Physiotherapy can be extremely effective in treating biceps tendonitis.
Our initial aim with physiotherapy treatment is to decrease the pain and inflammation around the tendon. Your physiotherapist may use electrical modalities for this purpose such as ultrasound or electrical current. Heat and/or ice can also be very useful in decreasing pain and inflammation so your therapist will encourage you to use heat or ice frequently at home; they can advise you on whether heat or ice is best for your particular injury. Your physiotherapist may also use massage around the shoulder, into the biceps muscle, and up into your neck area to ease your discomfort and assist with the associated inflammation.
A period of relative rest will also make a notable improvement in your shoulder pain. Relative rest indicates that you do not have to stop doing all activity, but rather that you stop or limit the amount of those activities that aggravate your shoulder. Resting your shoulder is crucial, along with simultaneous physiotherapy treatment, to calm the pain and inflammation associated with your injury.
Once the pain and inflammation are under control, your physiotherapy treatment will focus on regaining the range of motion, strength, and coordination in your shoulder. Your physiotherapist at Momentum Spine & Sport Physiotherapy will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of a home exercise program.
It is easiest to move the shoulder joint through its full range of motion if it is done passively, which means that you don’t use the muscles on your injured side to lift the shoulder. Your therapist may ask you to use a pole or a pulley in order to lift your arm up overhead or behind your back. If you do not maintain the motion in your shoulder by at least passively moving it through its full range of motion, it is easy for a frozen shoulder to develop. With a frozen shoulder the tissues in the shoulder actually shorten and tighten up such that anatomically the full shoulder range is no longer possible. All passive range of motion exercises prescribed should be done within the limits of pain, however there may be a mild discomfort as you reach the end of your range of motion, and this is normal. This mild discomfort is not detrimental to your progress so long as the pain remains at a very mild level. In some cases your physiotherapist themselves may move your shoulder for you in order to stretch it; again, this is considered passive motion. An upper body bike may also be useful in the early stages of rehabilitation to improve range of motion and encourage coordinated movement of the entire upper limb, as long as it can be used without causing more than mild discomfort.
A crucial component to any shoulder rehabilitation program is the ability for you to regain what is called ‘proprioceptive control’ of your shoulder joint. Proprioception is the ability to know where your body is without looking at it. For example, normally each time you reach overhead with your hand, your mind does not consciously have to think about doing the action, yet all of the muscles of the shoulder (and elbow, wrist, and upper back) coordinate the action just right so you can perform the movement without any discomfort or pinching. When you have pain in a joint, or the tissues of the joint have been injured, your proprioception declines. Any period of decreased mobility of the joint will also add to this decline. If the proprioceptive control of your shoulder is poor then the ability to use your shoulder naturally in all ranges of movement without causing any pain or pinching, or unnecessary motion, declines, and your shoulder is at risk of increased wear and tear, and developing another injury. The biceps tendon is very susceptible to feeling the effects of poor shoulder proprioception, and inflammation in the tendon can easily occur.
The joint between your shoulder blade and your thoracic spine (called the scapulothoracic joint) is particularly important to the overall proprioceptive control of the shoulder joint. The outer edge of the shoulder blade actually creates the socket of the shoulder joint. Together, the scapulothoracic joint and the shoulder joint itself (including the rotator cuff muscles) create the complete shoulder girdle; the entire shoulder girdle must operate together for normal shoulder motion. Controlled shoulder girdle motion along with adequate rotator cuff strength keeps the ball of the shoulder joint properly centered in the socket of the joint and avoids any pain or undesired motion of the joint. This centered position of the ball in the socket also keeps the ball of the shoulder joint from drifting forward and pressing on the biceps tendon, which causes unnecessary pressure and irritation. The control and strength of the scapulothoracic joint is particularly essential when using your limb is near or above shoulder height and especially during rapid or repetitive arm movements such as throwing.
For this reason, your physiotherapist will teach you how to properly control your shoulder girdle during your rehabilitation exercises but will also educate you on transferring this control to your everyday activities. Again, this will prevent excessive wear and tear on your shoulder joint even during the repetition of normal everyday tasks. Adequate control of the shoulder girdle is important to establish even before beginning any strengthening of the biceps muscle or the rotator cuff tendons.
In order gain the appropriate balanced strength in your rotator cuff muscles of the shoulder joint, as well as to address any biceps muscle weakness that may have developed your physiotherapist at Momentum Spine & Sport Physiotherapy will also prescribe strength specific exercises. Adequate strength in the rotator cuff can relieve pressure on the biceps tendon. Strength exercises may involve using light weights or Theraband to add resistance for your upper limb. As stressed above, an irritable biceps tendon can easily be made more irritable if your control and technique while performing strengthening exercises is poor, so your therapist will repeatedly focus on proper shoulder proprioception and exercise technique while you perform your exercises. Adequate strength and endurance in the rotator cuff muscles throughout a variety of ranges of motion, including above shoulder height, is needed to ensure full functioning of the shoulder.
As you improve with being able to control the shoulder girdle and as your strength improves your physiotherapist will introduce more difficult dynamic exercises for your shoulder. These may include exercises that simulate your daily tasks, or if you are a high-level athlete or particpate in recreational sport, those shoulder motions that simulate your sport. Simple proprioceptive exercises might include activities such as rolling a ball on a surface with your hand, holding a weight up overhead while moving your shoulder, or even doing push-ups on an unstable surface. Advanced exercises may include activities such as ball throwing, catching overhead, or a simulated swimming stroke or overhead volleyball spike.
Finally, as part of your shoulder rehabilitation, your physiotherapist will also remind you about maintaining good shoulder posture at all times even when just sitting or using your upper limb in activities below shoulder height, such as working on the computer. Rounded shoulders in any position crowds the shoulder joint and can lead to shoulder impingement, more pressure on the biceps tendon, poor recovery from your injury, or even the development of a new episode of shoulder pain. Simple changes in the way you sit or stand and how you use your shoulder, neck and thoracic spine throughout the day can ease your pain and help you avoid further problems.
In addition to rehabilitating your shoulder joint itself, at Momentum Spine & Sport Physiotherapy we highly recommend maintaining the rest of your body’s fitness with regular exercise even while you recover from the biceps tendonitis in your shoulder. Cardiovascular fitness can be maintained with lower extremity fitness activities such as walking or using a stationary bike or stepper machine. None of these exercises should cause discomfort to your shoulder; if they do, discuss modifying the activity with your physiotherapist.
You will notice improvements in the functioning of your shoulder even after just a few treatments with your physiotherapist at Momentum Spine & Sport Physiotherapy. If, however, your shoulder joint is not recovering as your % physiotherapist% would expect it should, or if your pain becomes unmanageable, your physiotherapist will suggest that you return to your doctor and/or see an Orthopaedic Surgeon. More radical treatment measures, such as surgery, may be needed in your case to deal with the problem.
Momentum Spine & Sport Physiotherapy provides services for physiotherapy in Edmonton and St Albert
 Welcome to Momentum Spine & Sport Physiotherapy's resource on biceps tendonitis.
Welcome to Momentum Spine & Sport Physiotherapy's resource on biceps tendonitis.
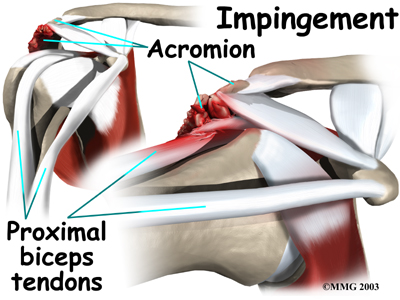

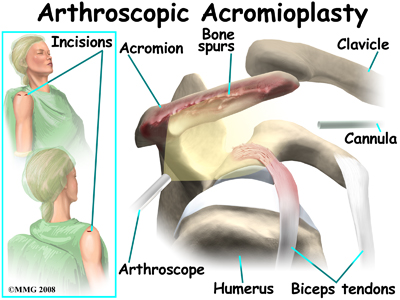 The most common surgery for bicipital tendonitis is acromioplasty, especially when the underlying problem is shoulder impingement. This procedure involves removing the front portion of the acromion, which is the bony ledge formed where the scapula meets the top of the shoulder joint. By removing a small portion of the acromion, more space is created between the acromion and the humeral head. This takes pressure off the soft tissues in between, including the biceps tendon.
The most common surgery for bicipital tendonitis is acromioplasty, especially when the underlying problem is shoulder impingement. This procedure involves removing the front portion of the acromion, which is the bony ledge formed where the scapula meets the top of the shoulder joint. By removing a small portion of the acromion, more space is created between the acromion and the humeral head. This takes pressure off the soft tissues in between, including the biceps tendon.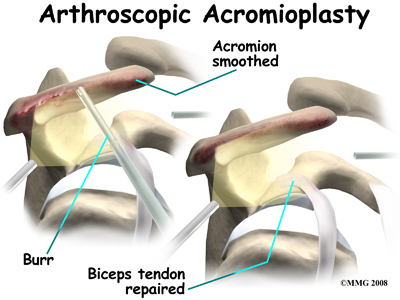 There are many small instruments that have been specially designed to perform surgery in the joint. Some of these instruments are used to remove torn and degenerative tissue. Some of these instruments nibble away bits of tissue and then vacuum them out of the joint. Others are designed to burr away and then vacuum up bone spurs that are rubbing on the tendons of the shoulder under the acromion.
There are many small instruments that have been specially designed to perform surgery in the joint. Some of these instruments are used to remove torn and degenerative tissue. Some of these instruments nibble away bits of tissue and then vacuum them out of the joint. Others are designed to burr away and then vacuum up bone spurs that are rubbing on the tendons of the shoulder under the acromion. 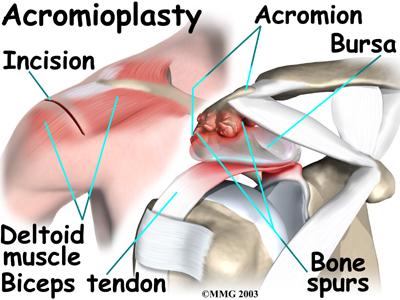
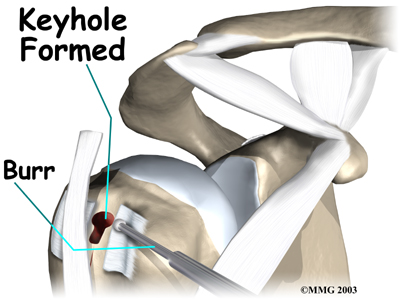
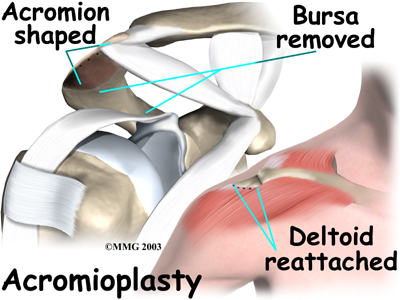 The surgeon then shaves the undersurface of the acromion to remove any bone spurs. A file is used to smooth the edge of the acromion. Next, a series of small holes are drilled into the remaining acromion. These holes are used to reattach the deltoid muscle to the acromion.
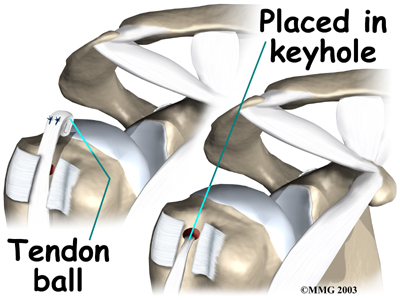
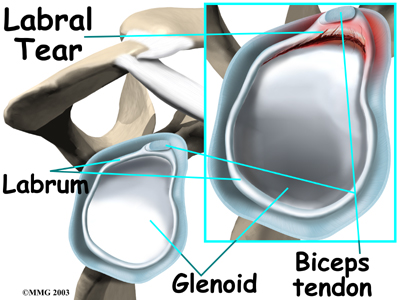
The surgeon then shaves the undersurface of the acromion to remove any bone spurs. A file is used to smooth the edge of the acromion. Next, a series of small holes are drilled into the remaining acromion. These holes are used to reattach the deltoid muscle to the acromion.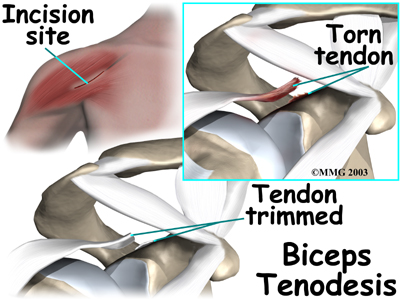 If the procedure is performed using the open method, however, the surgeon begins by making an incision on the front of the shoulder, just above the axilla (armpit). The overlying muscles are separated so the surgeon can locate the top of the biceps tendon. The end of the biceps tendon is removed from its attachment at the top of the glenoid. The tendon is prepared by cutting away frayed and degenerated tissue.
If the procedure is performed using the open method, however, the surgeon begins by making an incision on the front of the shoulder, just above the axilla (armpit). The overlying muscles are separated so the surgeon can locate the top of the biceps tendon. The end of the biceps tendon is removed from its attachment at the top of the glenoid. The tendon is prepared by cutting away frayed and degenerated tissue.