What should I expect after surgery?
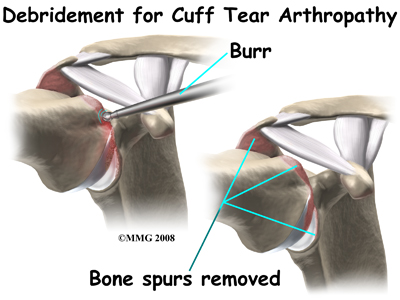
What you do for post-surgical rehabilitation depends on what type of surgery you have had. Those who have had a surgical debridement will require much less intense therapy than those who have had a full reverse shoulder arthroplasty. No matter which type of surgery you undergo, you will most likely require the use of a sling or shoulder brace after the surgery to protect your joint while it heals.
Generally after any type of surgery for rotator cuff arthropathy, a physiotherapist will see you in the hospital the day after surgery to begin your rehabilitation program. Your therapist will make sure you are safe when getting in and out of bed and moving about in your room with your sling on. Next, if your surgeon allows it, they will prescribe specific range of motion exercises for you. Your therapist will teach you how to remove your sling for your exercises and also how to put it back on after you have completed your exercises. After a major surgery such as the reverse shoulder replacement the sling should be worn at all times except during showering and while performing rehabilitation exercises.
When the immobilizer is removed following surgery, you will experience some pain when you start to move your shoulder, wrist, elbow and forearm. This pain is normal and is from not using the joints very efficiently previous to the surgery and also from the surgical process itself. The pain you feel with movement should only be mild to moderate and any sharp or severe pain should be heeded. In addition, after surgery the muscles in your arm may appear small and atrophied. Again, this is normal; once your strength begins to return your arm will start to look more normal again.
Simple finger, hand and wrist movements, as well as elbow and neck range of motion exercises will be prescribed to ensure you regain motion in these joints. Pendular exercises for your shoulder will be prescribed along with passive range of motion exercises that encourage shoulder elevation (raising in front) as well as gentle external rotation. Pendular exercises are performed by leaning forward or to the side, letting the arm hang clear of the chest, and then initiating movement with your trunk so that the dangling limb passively and gently moves. These exercises assist with pain, help to maintain some shoulder range of motion, and assist in preventing unwanted scar tissue forming in the joint. This pendular action also provides some traction to the glenohumeral joint, which aids in pain relief, and also assists the shoulder into a relatively elevated motion (in relation to the trunk). It is important that the pendular activity is done as passively as possible without initiating motion from the shoulder muscles. This exercise should be similar to a weighted pendulum that randomly swings on the end of a piece of string. Icing your shoulder will be encouraged after your exercises as well as several other times during the day.
Once you are managing your exercises well in the hospital, you are independent in doing most activities to care for yourself, and when your surgeon feels it is appropriate, you will be sent home. You will need to continue an extensive rehabilitation program once you are discharged from the hospital. In some cases, a physiotherapist or occupational therapist may visit your home to check to see that you are safely getting around within your home and managing your everyday tasks with your arm in your sling. Your therapist may also review and assist you with your exercises at this time. If it is particularly difficult for you to get out of your home to attend physiotherapy at Momentum Spine & Sport Physiotherapy then a physiotherapist may continue to visit you at your home for several treatments in order to review and advance your exercises. As soon as you are able, however, it is best for you to attend rehabilitation at Momentum Spine & Sport Physiotherapy as there are several more modalities as well as exercise equipment that can be used in the clinic versus at home, which can expedite your recovery.
As an initial goal of rehabilitation your physiotherapist at Momentum Spine & Sport Physiotherapy will focus on relieving your pain and decreasing any swelling that may be lingering from the surgery. We may use modalities such as heat, ice, ultrasound, or electrical current to assist with pain or decrease any swelling you have around your shoulder, anywhere along your arm, or into your hand. Due to some of the muscles of the neck and upper back connecting to the shoulder, you may also have pain in these regions, which we can also treat in order to make movement of your entire upper body easier. We may also use massage or mobilizations for the neck, upper back, shoulder, elbow, forearm, or wrist to improve circulation and assist with any pain that may be present.
If a reverse shoulder replacement has been done then protecting the new joint is of particular importance. Due to the biomechanics of a reverse arthroplasty there is a higher risk of shoulder dislocation than after a traditional shoulder replacement. With a traditional shoulder replacement the shoulder is more likely to dislocate with the arm in abduction and external rotation. With the reverse shoulder replacement dislocation is most likely during isolated extension as well as the combined movements of extension, internal rotation, and adduction therefore these movements should be avoided. Your therapist will review these movement precautions with you and you should refrain from putting your shoulder in any of these positions on their own or in combination for a minimum of 12 weeks post-surgically. Activities involving these positions, such as tucking in one’s shirt or performing personal hygiene of the back passage, are simple activities but can lead to dislocation so they must be strictly avoided. It can be helpful in respecting these precautions by remembering that you should always be able to see the elbow on your surgical side during all activities with that arm.
The next part of our post-surgical treatment will focus on regaining the range of motion, strength, and dexterity in your shoulder, elbow, hand and wrist. Your physiotherapist at Momentum Spine & Sport Physiotherapy will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of your home exercise program. These exercises may include the use of rehabilitation equipment such as pulleys and poles for range of motion exercises, and light weights or exercise bands for resistance work of your upper limb. The shoulder joint is the upper limb’s link to the rest of the body so it needs to be strong and well controlled for the limb and hand to work properly. If you have access to a pool your therapist may suggest you do some of your rehabilitation exercises in the pool where the warmth of the water and the hydrostatic properties of the water can be of assistance.
As time and range of motion progress, strengthening will become the major focus and will be advanced so that heavier weights or elastic bands are used and endurance of the muscles is improved. Your therapist will monitor your progress and advance your exercises as your shoulder can tolerate them. Along with more advanced strengthening exercises, active range of motion of the shoulder will be encouraged in order to assist with strengthening and control of the entire shoulder girdle.
Proprioception is the ability to know where your body is without looking at it. As a result of any injury or surgery, this ability declines in function. A period of immobilization adds to this decline. Although your arm and shoulder girdle are not traditionally thought of as weight-bearing parts of the body, even an activity such as assisting yourself with your arms to get out of a chair or pulling a glass from a cupboard requires weight to be put through or lifted by your shoulder girdle and for your body to be proprioceptively aware of your limb.
The proprioceptive control of the scapula on the rib cage (scapulothoracic motion) is especially important in being able to use your shoulder girdle and upper limb effectively without causing further injury. For this reason, your physiotherapist will teach you how to properly control your scapula during your rehabilitation exercises as well as during everyday activities. Your physiotherapist will also remind you about maintaining good shoulder posture at all times even when sitting or using your upper limb in activities below shoulder height, such as working on the computer. Rounded shoulders in this position crowds the shoulder joint and can lead to shoulder impingement and pain.
Regaining proprioception of the shoulder girdle and upper limb can require concentrated work, and most people have not previously needed to focus so intently on such controlled motions of this joint. The concentrated effort of shoulder rehabilitation, however, has a substantial reward; good scapulothoracic control is the key to regaining maximum shoulder girdle control and improved shoulder functioning while avoiding future shoulder pain.
Proprioceptive exercises might include activities such as rolling a ball on a surface with your hand, holding a weight up while moving your shoulder, or push-ups on an unstable surface. Advanced exercises may include activities such as ball throwing or catching. Exercises that simulate your everyday activities such as grooming yourself and getting dressed, in addition to those activities that simulate your work or hobbies will also be incorporated.
At Momentum Spine & Sport Physiotherapy we also highly recommend maintaining the rest of your body’s fitness with regular exercise while recovering from surgery. Several types of cardiovascular machines can be used such as a stationary bike, a stepper, or a treadmill for walking. Cardiovascular activity in a pool may also be appropriate. Your physiotherapist at Momentum Spine & Sport Physiotherapy can discuss when cardiovascular activity would be appropriate for you and which cardiovascular activity would be best. Most importantly, your surgical shoulder needs to be protected at all times so your therapist will educate you on how to do this.
Generally rehabilitation at Momentum Spine & Sport Physiotherapy after surgery for rotator cuff arthropathy goes smoothly. If, however, during rehabilitation your pain continues longer than it should or therapy is not progressing as your physiotherapist would expect, we will ask you to follow-up with your surgeon or doctor to confirm that the shoulder is tolerating the rehabilitation well and to ensure that there are no hardware issues that may be impeding your recovery.
Portions of this document copyright MMG, LLC.