What should I expect after surgery?
Rehabilitation at Momentum Spine & Sport Physiotherapy will begin as soon as your surgeon allows it. Each surgeon will set his or her own specific activity restrictions based on the surgical procedure used, their personal experience, and whether or not wrist is healing as expected.
Even while the cast is on and before extensive physiotherapy begins, at Momentum Spine & Sport Physiotherapy we highly recommend maintaining the rest of your body’s fitness with regular exercise. Activities such as walking or using a stationary bike or stepper machine are easy activities that can be done even while the wrist is healing. Avid runners may be able to continue running with clearance from their doctor. Weights or weight machines for your lower extremity and opposite arm are also acceptable to use as long as the restrictions regarding your healing wrist are strictly abided by. Lifting any weight at all with your injured side will not be allowed while your wrist is in the initial healing stages so you may require a friend to assist you with your workout if you are keen to continue during this time. Your physiotherapist at Momentum Spine & Sport Physiotherapy can discuss the most appropriate way for you to maintain your fitness while abiding by your doctor’s restrictions, and can provide a general fitness program specific to your needs.
When the cast is first removed after surgery you may experience some pain when you start to move your wrist, elbow and forearm. This pain is from not using the joints regularly while your wrist has been immobilized as well as from the surgical process itself. Your physiotherapist at Momentum Spine & Sport Physiotherapy will focus initially on relieving this pain. They may use modalities such as heat, ice, ultrasound, or electrical current to assist with decreasing any pain or swelling you have around the wrist or anywhere along the arm or into the hand. In addition, they may massage the hand, forearm, wrist, or elbow to improve circulation and assist with pain.
The next part of your treatment will focus on regaining the range of motion, strength, and dexterity in your wrist, hand, elbow, and shoulder. Your physiotherapist at Momentum Spine & Sport Physiotherapy will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of a home exercise program. These exercises may include the use of rehabilitation equipment such as pliable balls, exercise bands, or small weights that provide added resistance for your hand and wrist. Your physiotherapist may even give you exercises for your shoulder. The shoulder is the link of the upper limb to the rest of the body so it needs to be strong and well controlled for the upper extremity, particularly the wrist and hand, to work well. In addition, compensatory motions of the shoulder can affect how you use your wrist and lead to secondary pain in your shoulder.
The initial exercises prescribed will not require you to put any of your body weight through the wrist; you may simply be moving the wrist back and forth, side to side, turning your palm up and down, and rotating your wrist within the limits of pain. As your healing wrist allows, your physiotherapist will add in exercises where you are putting more stress through the wrist by taking the wrist into full ranges of motion, doing quick wrist motions, and doing eccentric strength exercises (see description under non-surgical rehabilitation). At the appropriate time your therapist will add in exercises where you are putting some of your body weight through your wrist via your hand, such as when pushing on a door or doing push ups against a wall.
Some patients have difficulty regaining pinch grip and grip strength after TFCC surgery so this will be addressed with specific exercises. Your therapist at Momentum Spine & Sport Physiotherapy will also focus particularly on gaining back those ranges of movement which are commonly lost after this type of surgery. These include ulnar deviation, supination, pronation, and wrist extension.
If necessary, your physiotherapist will mobilize your joints in order to gain range of motion. This hands-on technique encourages any stiff joints in your wrist, hand and elbow to move gradually into their normal range of motion.
As a result of any injury, the receptors in your joints and ligaments that assist with proprioception (the ability to know where your body is without looking at it) decline in function. A period of immobilization will add to this decline. Although your wrist is not traditionally thought of as a weight-bearing joint, even activities such as pushing up to get off of the couch, pulling a glass from a cupboard, or pushing a door open, require weight to be put through or lifted by your wrist and for your body to be proprioceptively aware of your limb. If you are active in sport, then proprioception of your upper extremity is paramount in returning you to your sport after surgery for a TFCC injury. Your physiotherapist at Momentum Spine & Sport Physiotherapy will prescribe exercises for you to regain this proprioception. These exercises may include activities such rolling a ball on a surface with your hand, holding a weight up overhead while moving your shoulder, or lightly tossing an item up and catching it. Advanced exercises wil
l include exercises such as ball throwing or catching overhead.
Fortunately, gaining range of motion, strength, and proprioception after surgery for a TFCC injury occurs fairly quickly. You will notice improvements in the functioning of your wrist even after just a few treatments at Momentum Spine & Sport Physiotherapy. As you improve, we will advance your exercises to ensure your rehabilitation is progressing as quickly as your healing wrist allows. Once your wrist can tolerate it, advanced exercises may include activities such as holding a push up position with your hands on a basketball, or dips in a chair where you are taking nearly your whole body weight through your wrist. It is crucial at each stage of rehabilitation to closely follow the instructions of your physiotherapist as the TFCC area can be easily aggravated if too much is done too quickly.
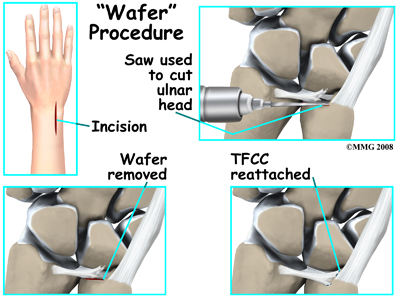
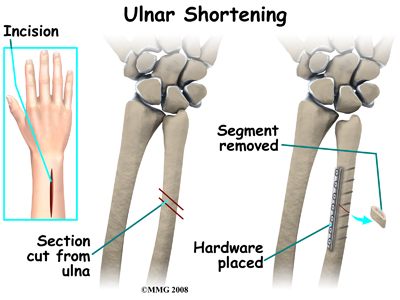
Generally, the wrist responds very well to the physiotherapy we provide at Momentum Spine & Sport Physiotherapy after surgery for a TFCC injury. Many patients are able to return to work with no restrictions. A small number of patients may require some work restrictions or permanent changes in work tasks. It should be noted, however, that in some cases complications such as persistent pain and stiffness occur. Your therapist will ask you to follow-up with your doctor if they feel your rehabilitation is not progressing as it should. Other complications such as infections, delayed union, or nonunion of bone fractures may also be a problem. In some cases further surgery may be needed to revise the first operation. Some patients need another surgery to remove any hardware used to stabilize the joint. In other cases the bottom of the ulna called the styloid may have to be removed. In rare cases, the procedure fails to provide the desired results and a wrist fusion may be the next step.
Portions of this document copyright MMG, LLC.
Momentum Spine & Sport Physiotherapy provides services for physiotherapy in Edmonton and St Albert.
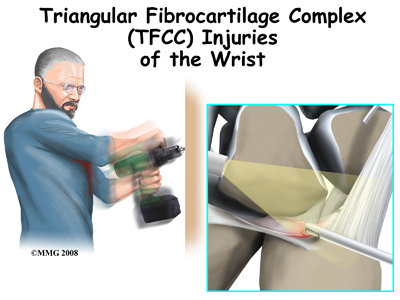
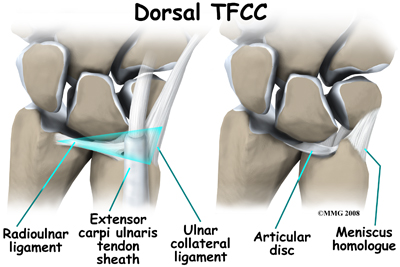
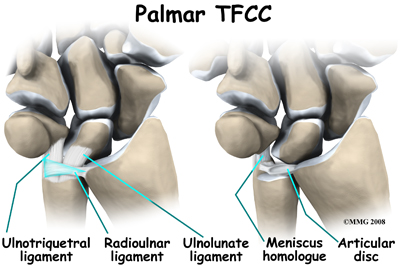
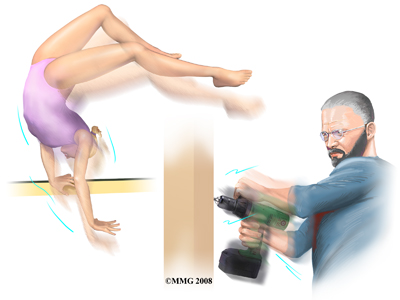 The TFCC stabilizes the wrist at the distal radioulnar joint. It also acts as a focal point for force transmitted across the wrist to the ulnar side. Traumatic injury or a fall onto an outstretched hand is the most common mechanism of injury. The hand is usually in a pronated or palm down position. Tearing or rupture of the TFCC occurs when there is enough force through the ulnar side of the hyperextended wrist to overcome the tensile strength of this structure.
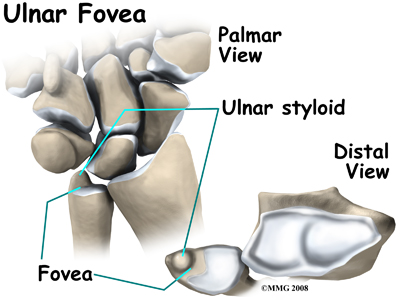
The TFCC stabilizes the wrist at the distal radioulnar joint. It also acts as a focal point for force transmitted across the wrist to the ulnar side. Traumatic injury or a fall onto an outstretched hand is the most common mechanism of injury. The hand is usually in a pronated or palm down position. Tearing or rupture of the TFCC occurs when there is enough force through the ulnar side of the hyperextended wrist to overcome the tensile strength of this structure.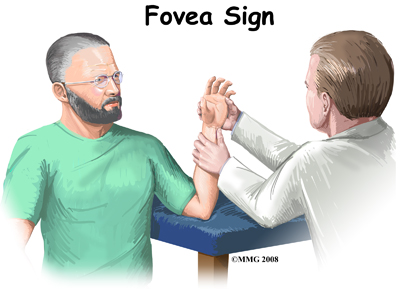 A new test called the fovea sign applies external pressure to the area of the fovea on the ulna bone. The examiner compares the involved wrist with the normal wrist. Tenderness and pain during this test is a sign that there may be a split-tear injury (down the middle length-wise) of the TFCC.
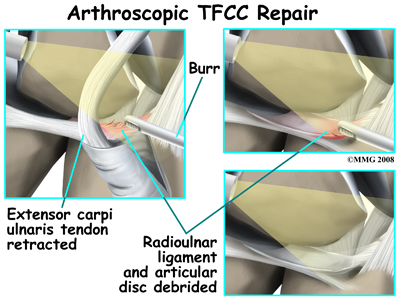
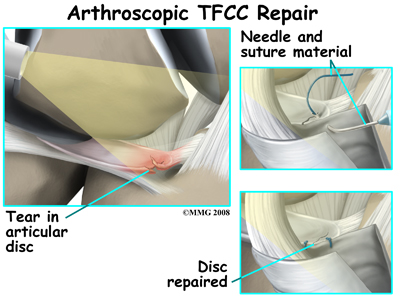
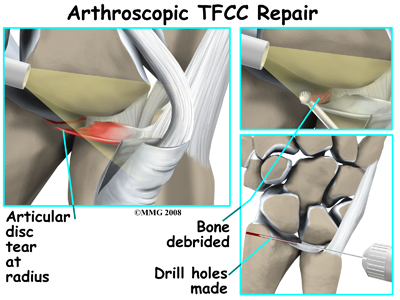
A new test called the fovea sign applies external pressure to the area of the fovea on the ulna bone. The examiner compares the involved wrist with the normal wrist. Tenderness and pain during this test is a sign that there may be a split-tear injury (down the middle length-wise) of the TFCC.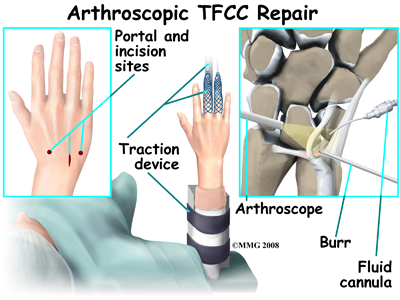 The outside perimeter of the TFCC has a good blood supply. Tears in this area can be repaired. There is no potential for healing when tears occur in the central area where there is no blood supply. In these cases arthroscopic debridement of the damaged tissue is required.
The outside perimeter of the TFCC has a good blood supply. Tears in this area can be repaired. There is no potential for healing when tears occur in the central area where there is no blood supply. In these cases arthroscopic debridement of the damaged tissue is required.